 胸腔急症~气胸
胸腔急症~气胸

《胸腔急症~气胸》由会员分享,可在线阅读,更多相关《胸腔急症~气胸(24页珍藏版)》请在装配图网上搜索。
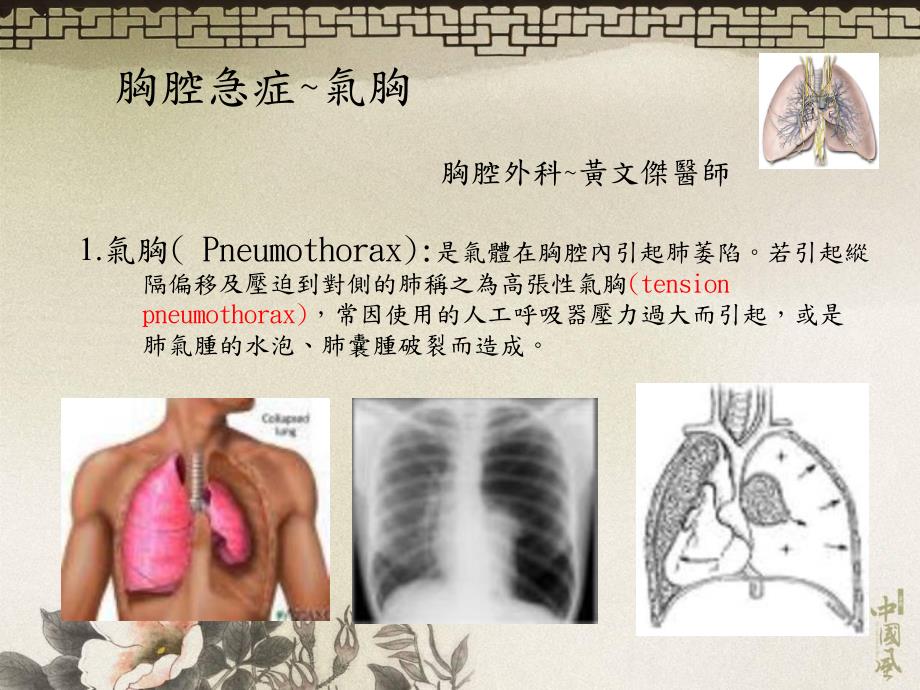
1、胸腔急症氣胸1.氣胸(Pneumothorax):是氣體在胸腔內引起肺萎陷。若引起縱 隔偏移及壓迫到對側的肺稱之為高張性氣胸(tension pneumothorax),常因使用的人工呼吸器壓力過大而引起,或是 肺氣腫的水泡、肺囊腫破裂而造成。胸腔外科黃文傑醫師診斷:i.理學檢查:患側的呼吸音減弱,心音偏向對側。有時頸部有捻 髮音(crepitus)。ii.胸部X光:患側呈現高透光性,而且沒有支氣管的顯影。旁邊 或甚至對側的肺葉萎陷。縱隔及心臟向對側偏移。治療:無症狀或僅有輕微的呼吸窘迫,可在病房作嚴密的看護,這種 單純性氣胸有三分之二在五至七天內自癒而無須手術。若有嚴重的呼吸困難及高張性氣胸
2、,則應立即採取行動。以靜 脈注射用之套管針,由前胸第二肋間或腋窩中線第五或第六 肋間插入,接上水下引流瓶,先解除呼吸困難。然後再改用 胸管插入,等肺完全擴張沒漏氣後24-48小時再拔除。手術(肺氣泡切除術、肋膜沾粘術)SpontaneousPrimarypneumothoraxSecondarypneumothoraxAirwayandpulmonarydisease(COPD,asthma)Interstitialdisease(Pulmonaryfibrosis)Infection(TB.)NeoplasticCatamenial(Endometriosis)IatrogenicPost-
3、TraumaticEarlycomplicationProlongedairleakageNonre-expansionofthelungBilateralityHemothoraxTensionCompletepneumothoraxPotentialhazardOccupationalhazardAbsenceofmedicalfacilitiesinisolatedareasAssociatedsinglebullaPsychologicalSecondEpisodeIpsilateralrecurrenceContralateralrecurrenceafterafirstpneumo
4、thoraxSurgicalindicationforprimaryspontaneouspneumothoraxSpontaneousPneumothorax-Definition&Factors DefinitionAccumulationofintrapleuralairastheresultofabreakineitherthevisceralorparietalpleura Factorsdetermininggasreabsorption Diffusionpropertiesofthegases Pressuregradients Areaofcontact Permeabili
5、tyofpleuralsurfaceSpontaneousPneumothorax-Clinicalinvestigation Signsandsymptoms Suddenonsetchestpain Shortnessofbreathing Cough Diagnosis CXR Auscultation Differentialdiagnosis Skinfold GiantbullaTreatmentOptionsforPneumothorax Observation Needleaspiration Percutaneouscathetertodrainage WatersealPl
6、eur-evactype Heimlichvalve Tubethoracostomy WatersealPleur-evactype Heimlichvalve Tubethoracostomywithinstillationofpleuralirritant Video-assistedthoracoscopicsurgery ThoracotomyIndicationsforSurgicalIntervention Secondepisode Persistentairleakageforgreaterthan7-10days Firstepisodewithunexpanded,“tr
7、apped”lung Historyofcontralateralpneumothorax Bilateralpneumothorax Occupationalrisk(driver,airplanepilot,livinginaremotearea)Largebulla Largeundrainedhemothorax Firstepisodeinapatientwithonelung FirstepisodeinapatientwithseverelycompromisedpulmonaryfunctionRecurrenceofPrimarySpontaneousPneumothorax
8、 TherapyRecurrence(%)Expectant30 Aspiration20-50 Chesttubedrainage20-30 Pleurodesis(tetracycline)25 Pleurodesis(talc)7 Surgery2ComplicationofPneumothorax Tensionpneumothorax Re-expansionpulmonaryedema Persistentairleak Hemothorax(lessthan5%)PneumomediastinumRemovalofChestTube Indications Nofluctuati
9、oninthefluidcolumnofthetube(completelungreexpansionortubeocclusion)Dailyfluiddrainage100mlin24hours Airleakagehasstopped Propertiming(controversy)Spontaneouspneumothoraxaftertubethoracostomy removaltubewithin6hoursofreexpansion-25%collapse TubeThoracostomy(ChestIntubation)IndicationofChestIntubation
10、Drainpleuralfluidorairpromotelungexpansion1.Pneumothorax2.Hydrothorax3.Hemothorax4.Chylothorax5.Pyothorax6.Post-thoracotomyetc.ApparatusofChestTubeDrainage1.Underwatersealedbottle:Separatefromatmosphere2.Collectingbottle:Decreaseresistanceofdrainage3.Negativepressuresuction:PromotelungexpansionProce
11、dureofChestIntubation1.Localanesthesia,confirmlocation2.Skinincisionatselectedarea3.Dissectintopleuralcavitythruasubcutaneoustunnel4.Deloculateinpleuralcavity5.Inserttubeposteriorlyandlaterally6.Closeincisionwound,fixedthetube7.Connecttubetounderwatersealedbottle(orwithnegativepressuresuction)Attent
12、ionInChestTubeInsertionAttentionPreventoccurrence1.ThruthoracostomywoundUnderlyingorganinjurypalpatetheunderlyingstructure(supra-orinfra-diaphragm)2.Avoidtrocarintubation(exceptLungorotherorganinjuryemergency)3.KeeptubeingooddirectionChestpain,greatvesselerosion4.AvoidintubationthruposteriorPain,una
13、bleinsupinechestwall5.Avoidtosuture&closeAirleakagethoracostomywoundtoolooseSkinnecrosis,painortootightAttentioninMassiveSubcutaneous(Mediastinal)Emphysema1.Keepairwaypatent(evenendotrachealtube)2.CXR3.Insertchesttubeinpneumothoraxorsuspiciousside4.Connecttubetonegativepressuresuctionimmediately5.Cl
14、osethoracostomywdslightlyloose6.Insertanothertubeifnoimprovement7.LowO2nasocannula8.Determinethecause&treatunderlyingdisease9.RemovetubeaftercompletesubsidenceWhentoRemoveChestTube?Criteria:1.Noairleakage2.Drainedfluid50c.c./day3.Clearserosanguineouscoloroffluid4.FullexpansionoflunginCXR Clearsteril
15、efluidremovedirectly Turbid,infectedfluidwithdrawprogressivelyopendrainAttentioninChestTubeCare(I)AttentionPreventoccurrence FixchesttubefirmlyTubemoving&contamination DontclamptubeduringTensionpneumothoraxtransportationinpresenceofairleakage DontusenegativepressuresuctionAbruptmediastinalshift,afte
16、rpneumonectomyvenousreturndecrease,death DontapplynegativesuctionReexpansionpulmonaryedemeimmediatelyafterintubationforcaseswithlargevolumeorlongdurationofpneumothorax,hydro-pyothoraxAttentioninChestTubeCare(II)AttentionPreventoccurrence DontliftuptubeaboveBackflowcontaminationthoracostomywound Usec
17、ollectingbottleandelevateBackflowcontaminationtheconnectingtubebetween2LungcollapsebottlesinbigresidualpleuralspaceormassiveairleakageAttentioninThoracotomywithLungResection(I)AttentionPreventoccurrence SutureligatedorclosepulmonarySlipout,bleedingvesselwithstapler MakeadequatelengthinbronchialStumpbrokenstump CoverbronchialstumpwithBronchopleuralfistulasurroundingtissue,especiallyinpneumonectomy Pre-operativeanti-TBoranti-fungalDiseaseflareupdrug(atleast2wks)forsuspiciousTBorfungaldiseases
- 温馨提示:
1: 本站所有资源如无特殊说明,都需要本地电脑安装OFFICE2007和PDF阅读器。图纸软件为CAD,CAXA,PROE,UG,SolidWorks等.压缩文件请下载最新的WinRAR软件解压。
2: 本站的文档不包含任何第三方提供的附件图纸等,如果需要附件,请联系上传者。文件的所有权益归上传用户所有。
3.本站RAR压缩包中若带图纸,网页内容里面会有图纸预览,若没有图纸预览就没有图纸。
4. 未经权益所有人同意不得将文件中的内容挪作商业或盈利用途。
5. 装配图网仅提供信息存储空间,仅对用户上传内容的表现方式做保护处理,对用户上传分享的文档内容本身不做任何修改或编辑,并不能对任何下载内容负责。
6. 下载文件中如有侵权或不适当内容,请与我们联系,我们立即纠正。
7. 本站不保证下载资源的准确性、安全性和完整性, 同时也不承担用户因使用这些下载资源对自己和他人造成任何形式的伤害或损失。
