 最新Cardiogenic ShockNT Cardiovascular Center:心源性休克 NT心血管中心文档资料
最新Cardiogenic ShockNT Cardiovascular Center:心源性休克 NT心血管中心文档资料

《最新Cardiogenic ShockNT Cardiovascular Center:心源性休克 NT心血管中心文档资料》由会员分享,可在线阅读,更多相关《最新Cardiogenic ShockNT Cardiovascular Center:心源性休克 NT心血管中心文档资料(53页珍藏版)》请在装配图网上搜索。
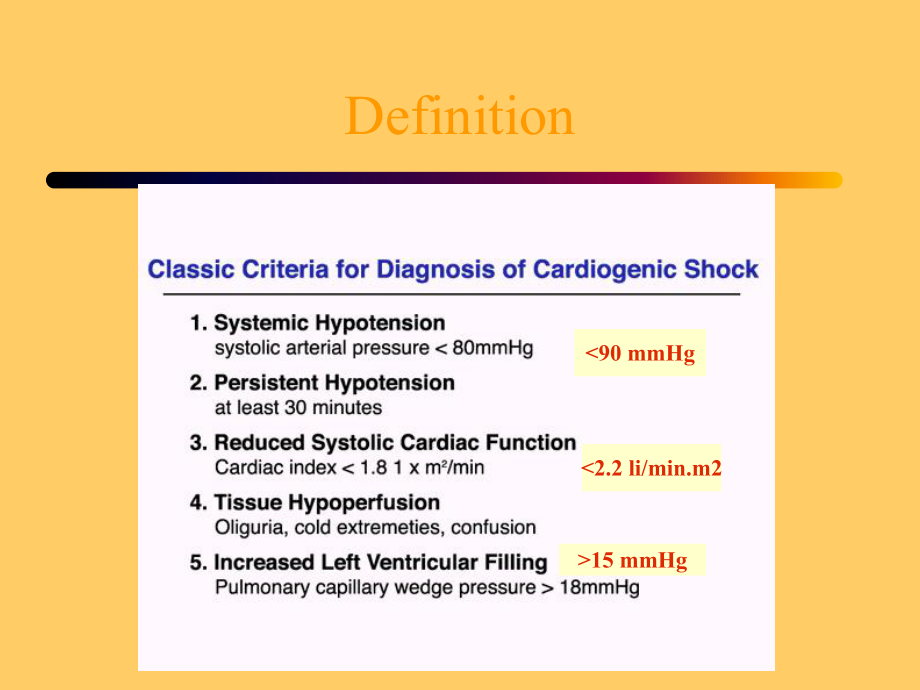
1、Definition90 mmHg15 mmHgSHOCK Registry JACC Sept.2000,Supp.A Spectrum of Clinical PresentationsMortalityRespiratoryDistressHypotensionHypoperfusion21%22%70%60%5.6%28%65%1.4%Risk Factors for Cardiogenic Shock Due to AMI-mediated LV DysfunctionAge 65Female genderLarge infarctionAnterior infarctionPrio
2、r infarctionDMPrior HTNPost-mortem study of Shock heartsAt least 40%of the myocardium infarcted in the aggregate(old and new injury)80%have significant LAD disease2/3 have severe 3VdzOutcomes of Cardiogenic ShockHistoric mortality 60-80%More recently reported mortality numbers 67%in the SHOCK trial
3、registry 56%in GUSTO-I(v.s.3%in Pts.without shock)Outcomes of Cardiogenic ShockThe ST pattern in Cardiogenic shock:15-30%Non-ST elevation MI Older Mortality:77%70-85%ST elevations MI/New LBBB Mortality:53-63%SHOCK registry findings on this pointOutcomes of Cardiogenic ShockThe SHOCK registry Similar
4、 mortality in the two groups 62.5%in non-ST elevation 60.4%with ST elevationPathophysiology of ShockEffect of Hypotension Flow in normal coronary:Regulated by microvascular resistance Coronary flow may be preserved at AO pressures as low as 50 mm Hg In coronary vessel with critical stenosis:Vasodila
5、tor reserve of microvascular bed is exhausted Decrease in AO pressure=Coronary hypoperfusionPathophysiology of ShockEffect of Hypotension(continued)Normal heart extracts 65%of the O2 present in the blood Little room for augmentation of O2 extractionPathophysiology of Shock Effect of:Elevated LVEDP o
6、n coronary flowLVEDP(mm Hg)Pathophysiology of ShockHypotension +LVEDP and critical stenosis Myocardial Hypoperfusion LV dysfunction Systemic lactic acidosis Impairment of non-ischemic myocardium worsening hypotension.SchematicLVEDP elevationHypotensionDecreased coronary perfusionIschemiaFurther myoc
7、ardial dysfunctionNeurohormonal activation VasoconstrictionEndorgan hypoperfusionMedical Stabilization of Shock Pts.Figure out the volume status,Swan if in doubt Air way Judicious afterload reduction Maintain AV synchrony Dont tolerate Afib Dual chamber pacing if A-V block present Correct Acid-Base
8、disturbances Maintain BP (IABP and/or Pressors).Physiologic Effect of IABP in-vivo Decreased afterload LV O2 consumption Williams,et.al.,Circulation 1982Kern,et.al.,Circulation 1993 Coronary blood flow velocity was measured using doppler-wire in nine patients with critical stenotic lesions.Peak dias
9、tolic coronary flow velocity beyond the stenosis was unaffected by intra-aortic balloon pumping.There was unequivocal IABP-mediated augmentation of both proximal and distal coronary blood flow velocities post PTCA.Physiologic Effect of IABP in-vivoFuchs,et.al.,Circulation,1983 Great cardiac vein flo
10、w was measured in seven patients receiving maximal drug therapy and requiring balloon pumping for unstable angina.All patients had greater than 90%stenosis of the proximal LAD coronary artery.Increased great cardiac vein flow correlated with increased mean aortic diastolic pressure across changes in
11、 balloon volumes(off,20 cc,30 cc,and 40 cc)and changes in assist ratio(off,1:4,1:2,and 1:1)(p=.02).Physiologic Effect of IABP in-vivoThus balloon pumping increased flow to a bed fed by the critical stenosis,or collateral vesselsIABP in Acute MIJACC 1985IABP in Acute MIqPre-thrombolytic eraqNo Lytics
12、,ASA,or Lopressorq20 patients with Acute MI and“extensive myocardium at risk per baseline Thalium”were Randomized.qPt.s in Shock were excludedStd.Rx:O2,MSo4,Lido,HeparinStd Rx+IABP Plus IV NTGIABP in Acute MIqPatients had repeat Thalium scan on Day-4qNo differences were observed between the two grou
13、ps regarding:-Thalium defect score comparing days 1 and 4-The ejection fraction comparing days 1 and 4=“Unlikely that a mortality benefit is conferred by the IABP/NTG combination”Utility of IABP in Shock Pts.Observed clinical benefits:Improved acid-base status Improved urine output Improved mentatio
14、n Improved overall hemodynamicsAll this,however,does not add up to improved survival without Flow RestorationThrombolysis in Cardiogenic ShockRates of Reperfusion Lower,andRates of Reocclusion HigherThan in non-shock ptsPossible Reason:Diffusion of thrombolytic agent into the thrombus may be PRESSUR
15、E DEPENDENT.BP Effect on efficacy of lytics in ShockDog data LAD occlusion by thrombus Hypotension induced by phlebotomyPrewittJACC 1994;23:784Any Randomized Trials ofThrombolysis in Cardiogenic Shock?Most thrombolytic trials specifically excluded patients in cardiogenic shockThe only large placebo-
16、controlled thrombolytic study specifically examining Pts.presenting with shock was GISSI-1 Streptokinase=No BenefitCombined IABP and ThrombolysisGUSTO-I:IABP in 62 of the 310 lytic Rxd Pts.in shockObservational Data:Combined IABP and Thrombolysis Kovack,et.al.,JACC 1997 Stomel,et.al.,Chest 1994Two r
17、etrospective observational series from community hospitals:Improved survival from combination Rx.Combined IABP and ThrombolysisObservational Data from SHOCK Registery:Combined IABP and Thrombolysis-Barron,et.al.,AHJ June 2001-National Registry of MI-2,Data base-21,178 pts.Presenting with or developi
18、ng post-MI shock-32%Received IABPP Selection BiasCombined IABP and ThrombolysisAccompanying Editorial by Magnus Ohman,and Judith Hochman:“Although,there is a wealth of physiologic and outcomes data to support the use of early IABP therapy in cardiogenic shock(in conjunction with lytics),randomized t
19、rials are clearly needed.”Combined IABP and ThrombolysisThe only randomized trial on the subject:Thrombolysis and Counterpusion to Improve Cardiogenic Shock Survival(TACTICS):Results of a Prospective Randomized Trial.Magnus Ohman,et.al.,Circulation Oct.2000 Supp.AbstractTACTICSqST elevation MI patie
20、nts,presenting within 12 hours of Sx,and Cardiogenic shockq57 Patients were randomizedThrombolyticTherapy aloneThrombolyticTherapy +IABPTACTICSqThe primary endpoint of 6 month mortality was not statistically significant,P=0.3qSubgroup analysis:For KILLIP classes III and IV,P=0.07PATIENT IS IN SHOCK
21、w/ST elevations,and 12 hrs Sx onset IABP PressorsMay increase the efficacy of LyticsAdministration of Lytics should not be delayed in anticipation of placement of IABPdespite lack of randomized data proving efficay.If EARLY REVASCULARIZATION is not to be pursued:SHOCK TrialWhether EARLY REVASCULARIZ
22、ATION improves survival among patients with cardiogenic shock?SHOCK Trial302 Pts.with ST elevation(or new LBBB)and cardiogenic shockImmediate Revascularization(CABG/PTCA)Late revascularization(if indicated)deferred for at least 54 hoursWithin 36 hrs.of MI onsetWithin 12 hrs.of Shock onsetSHOCK Trial
23、:Primary end point,30 days mortalityDiff.=9%P=0.1101020304050607030 days6 Months12 Months47%56%MortalityDiff.=13%P=0.02750%63%52.4%66.4%Diff.=14%P0.02Revasc.Med RxSHOCK TrialWhy wasnt the Primary end-point met?Low mortality in the initial medical mgt gp.High rates of IABP use,86%TT use,63%Delayed re
24、vasculariztion,21%Median of 104 hrspost randomization4244464850525456Early RevascMedical Mgt30 days mortality47%56%SHOCK Trial:Subgroup analysis,Age less than 7501020304050607030 days6 months12 MonthsRevasc.Med RxP=0.02CI1.0P=0.002CI1.0Mortality45%65%41%56%66.7%48.4%P0.02CI 1.0)6 months(CI 1.0)12 mo
25、nths,no difference in outcomeWhat to do with Pt.s older than 75SHOCK Registry results is in contrast to the SHOCK Trial findings in this subgroup.Those older than 75 y.o.,selected to undergo ERV had a survival advantage.Case by case assessment in this population,and not across the board exclusion is
26、 called for.Role of IIb/IIIa Inhibitors and Stents in Cardiogenic ShockqSHOCK Trial:Revascularization(N=152)Medical Treatment(N=150)IIb/IIIa Antagonist41.7%25%Stent Placement35.7%52.3%Role of IIb/IIIa inhibitors in Cardiogenic Shock q Retrospective subgroup analysis from the PURSUIT trialHassade,et.
27、al.,JACC,2000 Randomization to eptifibatide did not affect the incidence of shock Patients randomized to eptifibatide who developed shock had a significantly reduced incidence of death at 30 days A possible mechanism of benefit is relief of microvascular obstructionRole of IIb/IIIa Inhibitors and St
28、ents in Cardiogenic ShockLong-Term Mortality Benefit With the Combination of Stents and Abciximab for Cardiogenic Shock Complicating Acute Myocardial InfarctionCoronary Artery DiseaseChan,Albert W.MD,MS;Chew,Derek P.MBBS;Bhatt,Deepak L.MD;Moliterno,David J.MD;Topol,Eric J.MD;Ellis,Stephen G.MDAJC Ja
29、n.15,2002Role of IIb/IIIa Inhibitors and Stents in Cardiogenic ShockSingle center,non-randomizedData collected:Jan.1993 and June 2000 Thirty month follow-up available96 Pt.s w/Cardiogenic ShockStent+ReoproN=27Stent OnlyN=14PTCA+ReoproN=18PTCA OnlyN=37Role of IIb/IIIa Inhibitors and Stents in Cardiog
30、enic ShockThirty day Mortality Rates(%)010203040506070EastStent+ReoproStent OnlyPTCA+ReoproPTCA OnlyAbsence of Stent use:HR 2.39,95%CI 1.22 to 4.67,p=0.01Absence of Abciximab use:HR 1.95,95%CI 1.03 to 3.71,p=0.04On Univariate analysis:EF=30%HR 3.44,95%CI 1.35 to 8.78,p=0.01Role of IIb/IIIa Inhibitor
31、s and Stents in Cardiogenic ShockUse of Stents29%Absolute mortality reduction1 additional life saved for each 3-4 treated Patients.Abciximab+Stenting10%Absolute mortality reduction 1 additional life saved for each10 patients treated.At 30 monthsRole of IIb/IIIa Inhibitors and Stents in Cardiogenic S
32、hock Results of Primary Percutaneous Transluminal Coronary Angioplasty Plus Abciximab With or Without Stenting for Acute Myocardial Infarction Complicated by Cardiogenic ShockCoronary Artery DiseaseGiri,Satyendra MD,MPH,MRCP;Mitchel,Joseph DO;Azar,Rabih R.MD,MSc;Kiernan,Francis J.MD;Fram,Daniel B.MD
33、;McKay,Raymond G.MD;Mennett,Roger MSc;Clive,Jonathan PhD;Hirst,Jeffrey A.MD,MSAJC,15 January 2002 .Role of IIb/IIIa Inhibitors and Stents in Cardiogenic ShockThis was a nonrandomized,prospective observational study.113(13.9%)were diagnosed with cardiogenic shock from 8/95 to 8/99.Role of IIb/IIIa In
34、hibitors and Stents in Cardiogenic ShockNo ReoproWith ReoproRole of IIb/IIIa Inhibitors and Stents in Cardiogenic ShockMultivariate AnalysisRole of IIb/IIIa Inhibitors and Stents in Cardiogenic ShockSpeculation:Greater use of Abxicimab,and Stents in the SHOCK Trial may well have resulted in a positi
35、ve primary endpoint.The age cutoff of 75 may or may not have retained its significance vis-vis increased mortality.Reversal of Cardiogenic Shock by Percutaneous Left Atrial-to-Femoral Arterial Bypass Assistance Holger,et.al,Circulation.2001;104:2917.VADs were implanted in 18 consecutive patients who
36、 had cardiogenic shock after myocardial infarction A 21F venous cannula into the left atrium by transseptal puncture using TEE Pts served as their own controls All hemodynamic parameters showed significant improvement“The influence of this device on long-term prognosis warrants further investigation
37、.”Take Home PointsCombining Reopro with Stenting is likely to enhance the benefit of early revascularization.IABP helpful in stabilizing the Pt.Mitigates clinical signs of SHOCK May improve outcome with concurrent LyticsNo definitive evidence(randomized trials)showing improved outcomes with IABP/Lyt
38、ic combinaiton.Take Home PointsNothing magical about the age cut off of 75,case by case assessment in this population is called for.If pt.is not a candidate for early revascularization,but is within12 hrs.of MI onset,administration of lytics(subject to risk-benefit assessment,age,grafts,)should not be delayed in anticipation of placement of IABP.
- 温馨提示:
1: 本站所有资源如无特殊说明,都需要本地电脑安装OFFICE2007和PDF阅读器。图纸软件为CAD,CAXA,PROE,UG,SolidWorks等.压缩文件请下载最新的WinRAR软件解压。
2: 本站的文档不包含任何第三方提供的附件图纸等,如果需要附件,请联系上传者。文件的所有权益归上传用户所有。
3.本站RAR压缩包中若带图纸,网页内容里面会有图纸预览,若没有图纸预览就没有图纸。
4. 未经权益所有人同意不得将文件中的内容挪作商业或盈利用途。
5. 装配图网仅提供信息存储空间,仅对用户上传内容的表现方式做保护处理,对用户上传分享的文档内容本身不做任何修改或编辑,并不能对任何下载内容负责。
6. 下载文件中如有侵权或不适当内容,请与我们联系,我们立即纠正。
7. 本站不保证下载资源的准确性、安全性和完整性, 同时也不承担用户因使用这些下载资源对自己和他人造成任何形式的伤害或损失。
